































































Modernit sisustukset käyttävät valoa paljon muuhun kuin näkyvyyteen; valaistus toimii nyt ympäristön signaalina, joka muokkaa huomiota, mielialaa ja ihmisen biologista kelloa. Markkinoilla kuitenkin kaksi hyvin erilaista kategoriaa sekoitetaan usein: tunnelmavalaistus, joka luo ilmapiiriä, ja kliininen valohoito, joka on suunniteltu siirtämään vuorokausirytmiä ja vakauttamaan mielialan fysiologiaa. Markkinointikieli usein hämärtää rajaa, esimerkiksi ”pehmeä iltahohde paremman unen puolesta” tai ”energisoiva päivänvalovaikutus”, vaikka laitteelta puuttuisi biologiseen vaikutukseen vaadittu intensiteetti, spektri ja ajoitusprotokollat. Koristevalon ja hoidon erottaminen ei ole pelkkä sanallinen nyanssi vaan valohygienian kulmakivi, koska rutiinit joko tukevat tervettä unta tai heikentävät sitä huonosti ajoitetun ja riittämättömän valon altistuksen kautta (Harvard Health, 2023 Czeisler et al., 2019.)
Vastaavan tärkeää on ymmärtää tarkoitus ja ajoitus. Koristevalo on joustavaa: lämpimät, himmeät valonlähteet illalla vähentävät silmien rasitusta, rentouttavat hermostoa ja tekevät tiloista turvallisia ja intiimejä. Terapeuttinen valo on kurinalaista: korkea valaistusvoimakkuus, sinisellä rikastettu valkoinen valo annetaan pian heräämisen jälkeen melatoniinin estämiseksi, vuorokausirytmin aikaistamiseksi ja aamuvireyden lisäämiseksi. Sama fyysinen ärsyke väärään aikaan voi kääntyä itseään vastaan, koska kirkas, viileä valo myöhään päivällä viivästyttää nukahtamista, siirtää sisäistä kelloa myöhäisemmäksi ja pirstoo unen rakennetta (Cajochen ym., 2019 Sleep Medicine Reviews, 2022.)
Keskeiset opit: esteettinen valo ei ole terapeuttinen annos; tehokas valohoito kohdistuu ipRGC–SCN-reittiin riittävällä luksilla, spektrillä ja aamun ajoituksella; ja kestävät tulokset riippuvat säännöllisestä aamun altistuksesta sekä kirkkaan, lyhytaaltoisen valon hillitsemisestä illalla (National Sleep Foundation, 2022 Reid ym., 2018.)

Mitä ”Tunnelmavalaistus” käytännössä tarkoittaa
Tunnelmavalaistus on tunnepohjaisen muotoilun väline. Se muokkaa värilämpötilaa, suuntaa ja hajotusta muuttaakseen huoneen tunnelmaa esimerkiksi kodikkaaksi, intiimiksi, leikkisäksi tai moderniksi. Tyypillinen silmien valaistusvoimakkuus on alle 500 luksi, kaukana ulkoilman päivänvalon tasosta ja alle terapeuttisten kynnysten. Lämpimät sävyt noin 2700–3000 K suositaan rentoutumiseen ja nukahtamisen valmisteluun, kun taas kylläiset RGB-kohtaukset tukevat estetiikkaa tai kokemuksellisia vaikutuksia. Havaittavat hyödyt ovat todellisia, koska vähentynyt karheus ja pehmeämpi kontrasti luovat rauhallisemman ilmapiirin, mutta ne toimivat pääasiassa psykologisten kanavien kautta eivätkä vuorokausirytmin fysiologian kautta (Baselin yliopisto, 2020 Harvard Health, 2023.)
Todellisissa kodeissa ja toimistoissa mielialavalaistus toimii kerroksena toiminnallisen valaistuksen päällä: pöytävalaisimet, jotka valaisevat seiniä, LED-nauhat, jotka korostavat arkkitehtonisia yksityiskohtia, meripihkanväriset hehkulamput, jotka alentavat vireystilaa oleskelutiloissa, ja älylamput, jotka tallentavat suosikkikohtauksia. Nämä elementit parantavat mukavuutta ja visuaalista ergonomiaa erityisesti yöllä, kun korkean korreloidun värilämpötilan valo voi tuntua kliiniseltä tai aktivoivalta. Koska valon intensiteetti on maltillinen ja spektrit usein poikkeavat taivaansinisen alueelta, mielialavalaistus ei aktivoi verkkokalvon melanopsiinia tarpeeksi siirtääkseen kehon kelloa tai merkittävästi estääkseen melatoniinia. Se täydentää sisustusta; se ei hoida unihäiriöitä (Reid ym., 2018.)
Yleisiä mielialavalaistustyyppejä ovat RGB-LED-nauhat ja -paneelit värikohtauksia varten, meripihkanväriset vintage-lamput noin 2200–2400 K, älylamput rentoutusasetuksilla, koristeelliset seinäkynttilät ja lyhdyt, suolalamput sekä pehmeät hajavalaisimet työpöydille.
Tyypilliset tuotteet ja käyttötarkoitukset
Kotitalouksissa käytetään RGB-valonauhoja televisioiden ja sängynpäätyjen takana visuaalisen dramatiikan luomiseksi, meripihkanvärisiä lasilamppuja olohuoneissa häikäisyn vähentämiseksi sekä älylamppuja, jotka himmentyvät hitaasti ennen nukkumaanmenoa. Hotellit käyttävät lämpimiä seinävalaisimia ja seinäkynttilöitä ohjatakseen asiakkaita rauhalliseen keskusteluun. Peliasetuksissa suositaan voimakkaita värejä immersioelämyksen lisäämiseksi. Nämä laitteet optimoivat havaintoa, eivät vuorokausirytmin säätelyä, joten ne ovat erinomaisia kumppaneita iltarutiineihin, joissa halutaan matalaa vireystilaa (Baselin yliopisto, 2020.)
Käyttötapauksiin kuuluvat lukupaikat 2700 K lampuilla, yöpöydän meripihkanväriset yövalot, jotka häiritsevät melatoniinia mahdollisimman vähän, lämpimät seinävalaisimet viihtyisiin oleskelutiloihin, RGB-valaistus viihdealueille ja pehmeä käytävävalaistus yöaikaisen häikäisyn vähentämiseksi.
Miksi mielialalamput eivät siirrä sisäistä kelloasi
Vuorokausirytmin säätely perustuu silmän sisäisesti valolle herkkien verkkokalvon gangliosolujen toimintaan, jotka reagoivat voimakkaasti sinisellä rikastettuun valoon aallonpituudella 460–480 nm, kun valo on riittävän voimakasta ja biologisesti merkityksellisen ajan kestävä. Mielialalamput epäonnistuvat yleensä vähintään kahdella osa-alueella: silmään kohdistuva valon määrä (luksit) on riittämätön ja spektriprofiilit on suunniteltu tunnelmaa varten eivätkä melanopista tehokkuutta ajatellen. Ilman riittävää annosta, joka merkittävästi stimuloi ipRGC-SCN-reittiä, huone näyttää kauniimmalta, mutta melatoniinin eritys ei aikaistu eikä kehon ydinlämpötilan minimi siirry aikaisemmaksi. Lyhyesti sanottuna mielialalamput muuttavat tuntemustasi huoneesta, eivät kehosi ajanmittausta (Cajochen ym., 2019 Czeisler et al., 2019.)
Kliinisen valohoidon perusteet
Kirkasvaloterapia on kliininen hoitomenetelmä, joka käyttää kontrolloitua, korkean intensiteetin, sinisellä rikastettua valkoista valoa vaikuttaakseen vuorokausirytmin vaiheeseen ja mielialan säätelyyn. Todisteet alkoivat kaamosmasennuksesta ja ovat laajentuneet viivästyneen univalverytmin häiriöön, aikaerorasitukseen sekä lisähoitona kausittomassa masennuksessa. Oikein ajoitetut aamun istunnot estävät melatoniinin eritystä, lisäävät kortisolia sen luonnollisessa huipussaan ja siirtävät vaihetta aikaisemmaksi, parantaen unen ajoitusta, vireyttä ja päivävireyttä (Lam ym., 2016 Lewy ym., 2018.)
Keskeiset merkitykselliset parametrit ovat valaistusvoimakkuus tyypillisesti 2 000–10 000 luksista silmään, spektri, jossa on vahva melanopinen sisältö, ajoitus noin 30–60 minuuttia heräämisen jälkeen, kesto noin 20–45 minuuttia ja geometria, joka vakauttaa verkkokalvon annoksen ilman häikäisyä. Kun nämä täyttyvät, tulokset ovat luotettavia; kun ne ovat puutteellisia, kuten liian himmeä, liian myöhäinen tai liian lyhyt, hoito ei tehoa tai jopa viivästyttää kelloa (Sleep Medicine Reviews, 2022 National Sleep Foundation, 2022.)
Kliinisen hygienian tee ja älä: Käytä aamuajoitusta, istu valmistajan määrittämällä etäisyydellä, pidä silmät avoimina ja vilkaise ajoittain valonlähteeseen, toista päivittäin. Älä käytä kirkasta terapiavaloa myöhään iltapäivällä tai illalla, älä venytä sessioita korvataksesi menetettyjä päiviä, äläkä oleta, että mielialalamput voivat korvata terapeuttisen annoksen.
Indikaatiot ja näyttöjen yleiskatsaus
Indikaatiot sisältävät kaamosmasennuksen, myöhäisen univaiheen häiriön, sirkadiaanisen epäsynkronian vuorotyössä ja jet lagissa, kognitiivisen suorituskyvyn tukemisen vähäisessä päivänvalossa sekä tukevat roolit ei-kausiluonteisessa masennuksessa kliinisen valvonnan alaisena (Lam ym., 2016 Sleep Medicine Reviews, 2022.)
Tutkimukset osoittavat, että kirkas aamuvalo vähentää kaamosmasennuksen oireita, aikaistaa uniaikaa myöhäisen univaiheen häiriössä noin 1–2 tuntia ja parantaa valppautta vähemmän päivänvaloa saaneilla, kuten toimistotyöntekijöillä ja korkeilla leveysasteilla asuvilla. Vaikutuksen suuruus riippuu sitoutumisesta, annoksesta ja myöhäisen illan kirkkaan valon estosta (Lewy ym., 2018 Reid ym., 2018.)
Annosteluparametrit, joilla on todellista merkitystä
Mielialavalaistus vs. terapia: Tärkeä rinnakkainen vertailu
Ennen valopohjaisen rutiinin omaksumista, perusta odotukset objektiivisiin eroihin. Sisustus optimoi tunnelman ja mukavuuden; terapia kohdistuu biologiaan ja ajoitukseen. Alla olevan taulukon lukeminen tarkistuslistana estää väärinymmärryksiä, kuten tyylikkään lampun ostamisen kliinisen tuloksen saavuttamiseksi, johon se ei pysty (Sleep Medicine Reviews, 2022.)
Kriteeri |
Mielialavalaistus (Sisustus) |
Valoterapia (Kliininen) |
Pääasiallinen tarkoitus |
Tunnelma ja visuaalinen mukavuus |
Sirkadiaaninen vaiheensiirto ja mielialan säätely |
Tyypillinen valaistusvoimakkuus |
Alle 500 luksista silmään |
2 000–10 000 luksia silmään |
Spektri |
Lämmin tai RGB, esteettinen |
Sinistä valoa sisältävä valkoinen, melanopisesti tehokas |
Käytön ajoitus |
Joustava, usein illalla |
Tiukasti aamulla heräämisen jälkeen |
Odotettu tulos |
Koettu rentoutuminen ja miellyttävyys |
Melatoniinin erityksen väheneminen, vaihe-ennakointi, vireystila |
Protokolla |
Ei mitään, kohtausidonnainen |
20–45 min, päivittäin, toistettava geometria |
Taulukon tulkinta: Mitä kukin rivi tarkoittaa
Miten valo kommunikoi aivojen kanssa
Ihmisen vuorokausirytmiä säätelee suprachiasmaattisen tumakkeen mestaritahdistin, joka synkronoituu päivittäin verkkokalvon valosignaalien avulla. Erityiset melanopsiinia sisältävät intrinsisesti valolle herkät verkkokalvon gangliosolut projisoivat retinohypotalamuksen kautta suprachiasmaattiseen tumakkeeseen, joka koordinoi hormonirytmejä kuten melatoniinia ja kortisolia, kehon ydinlämpötilaa ja univalvetilaa. Aamun sinistä valoa sisältävä valo nopeuttaa kelloa vaihe-ennakoinnilla, kun taas myöhäinen illan sininen valo viivästyttää sitä, siirtäen unta myöhemmäksi ja heikentäen hitaiden aaltovaiheiden konsolidointia (Czeisler et al., 2019 Cajochen ym., 2019.)
Käytännön merkitys on, että annos ilman ajoitusta on tehoton. Kymmenen minuuttia 10 000 luksin valoa keskipäivällä ei vastaa 30–40 minuuttia ensimmäisen tunnin aikana heräämisen jälkeen. Samoin johdonmukainen illan lyhytaaltoisen valon himmennys moninkertaistaa vaikutuksen, koska se suojaa aamun hyötyjä sallimalla melatoniinin erityksen alkaa ajallaan. Monet kotitaloudet tuhoavat tiedostamattaan aamun hyödyt käyttämällä kirkasta työvaloa tai näyttöjä auringonlaskun jälkeen (Reid ym., 2018 Harvard Health, 2023.)
Reitin vaiheet yksinkertaistettuna: 1) sinistä valoa sisältävät fotonit saavuttavat ipRGC:t, 2) signaalit kulkevat suprachiasmaattiseen tumakkeeseen, 3) kello siirtää geeniekspression ajoitusta, 4) melatoniinin eritys vähenee ja kortisolin rytmi kohdistuu, 5) aikaisempi univalmius ja parantunut aamuvireys seuraavat.
ipRGC:n ja SCN:n välinen reitti yksinkertaistettuna
Ajattele ipRGC-soluja valon aikahavaitsijoina. Ne eivät muodosta kuvia, vaan välittävät aivoille tiedon päivänvalosta. Riittävällä aamun valostimulaatiolla sisäinen tahdistin kohdistaa solukellot koko kehossa keskuksesta ääreisalueille, vakauttaen ruokahalun rytmit, lämpötilan minimin ja kognitiiviset huiput. Riittämätön aamun valostimulaatio aiheuttaa sisäistä viivästymää, joka kasaantuu myöhäisiin nukkumaanmenoihin, vaikeisiin heräämisiin ja sosiaaliseen jetlagiin (Czeisler et al., 2019 Roenneberg et al., 2012.)
Ajoitusikkunat: Aamun aikaistuminen vs Illan viivästyminen
Kuinka tunnistaa aito terapiaväline ja välttää näennäiset
Kuluttajamarkkinoilla on monia hyvinvointilamppuja, jotka esittävät terapeuttisia väitteitä. Aito terapiaväline on tarkka annoksesta, geometriasta, turvallisuudesta ja ajoituksesta. Käytä tätä tarkistuslistaa suodattimena ennen ostoa ja noudattamisen työkaluna jälkeenpäin.
Vaadittavien asioiden tarkistuslista: silmien tasolla vähintään 2 000 luksia määritellyllä etäisyydellä ja kulmalla, sinistä rikastettu valkoinen tai melanooppisesti tehokas spektri ja UV-vapaa teho, aamun ajoitusohjeet istunnon kestolla, vakaa geometria tasaisen verkkokalvon annoksen varmistamiseksi, turvallisuusohjeet kuten häikäisyn hallinta ja silmävaroitukset, sertifiointi kuten CE tai FDA-luokka tarpeen mukaan, sekä käyttäjäohjeet annoksen asteittaisesta vähentämisestä tai ohjeet ohitetun päivän käsittelyyn (National Sleep Foundation, 2022 Sleep Medicine Reviews, 2022.)
Markkinoinnin punaiset liput ovat esimerkiksi ”lisää energiaa” ilman luks-arvoa tai etäisyystietoa, RGB-hoitotilat, kirkkaan valkoiset illan unta edistävät esiasetukset, turvallisuus- tai sertifiointitietojen puute, koristekuvat ilman protokollakieltä ja epämääräinen ajoitus kuten ”käytä milloin tahansa.” Nämä viestit viittaavat yleensä sisustukseen, joka naamioituu terapiaksi (Reid ym., 2018.)
Toimivat rutiinit: Aamun valo osaksi arkea
Suunnittele protokollasi heräämisaikasi mukaan, älä pelkästään kellonajan. Paras käytäntö on aloittaa 30–45 minuutin kuluessa heräämisestä, yhdistää istunto tavanomaiseen rutiiniin kuten aamiaiseen tai sähköpostin läpikäyntiin ja pitää kesto tasaisena 20–40 minuutissa. Vahvista lyhyellä ulkovalotauolla, jos mahdollista, sillä jopa varjostettu päivänvalo sisältää melanooppista valoa, jota ei ole sisätiloissa. Illalla himmennä valaistus lämpimäksi ja poista suorat sinisen valon lähteet 1–2 tuntia ennen nukkumaanmenoa. Nämä kaksi toimenpidettä, aamun valoannos ja illan suojaus, tuottavat suhteettoman hyviä tuloksia vaivaan nähden (National Sleep Foundation, 2022 Harvard Health, 2023.)
7 vaiheen aloitussuunnitelma yhdelle viikolle: 1) kiinnitä heräämisaika plus- tai miinus 15 minuutin ikkunaan, 2) aloita valohoito 30–45 minuutin kuluessa ja tee 25–35 minuuttia per istunto, 3) pidä laite määritetyllä etäisyydellä ja kulmassa ja pidä silmät luonnollisesti avoinna, 4) yhdistä rutiinitehtävään sitoutumisen automatisoimiseksi, 5) lisää aamupäivällä 5–10 minuutin ulkovalotauko, jos mahdollista, 6) auringonlaskun jälkeen käytä lämpimiä ja himmeitä valaistuksia ja rajoita näyttöjä, 7) viikko viikolta siirrä nukkumaanmenoaikaa 10–15 minuuttia aiemmaksi unenpaineen kasvaessa (Roenneberg et al., 2012 Reid ym., 2018.)
Kannettava valohoito: Miksi hoidon noudattaminen muuttaa kaiken
Paikallaan olevat valolaatikot perustuvat näyttöön, mutta ovat ergonomisesti jäykkiä, koska istut paikallasi, kohtaat paneelin ja odotat. Kiireisissä kodeissa ja nuorten keskuudessa hoidon noudattaminen heikkenee, koska hoito kilpailee aamun logistiikan kanssa. Kannettavat ratkaisut poistavat geometriaongelman tuomalla valon silmien lähelle hallitussa kulmassa samalla kun liikkuvuus säilyy, mikä muuttaa hoitohetket kädet vapaana olevaksi rutiiniajaksi. Parempi hoidon noudattaminen ei ole vain mukavuustekijä, sillä se usein erottaa tilastolliset ja kliiniset vaikutuskoot (Sleep Medicine Reviews, 2022.)
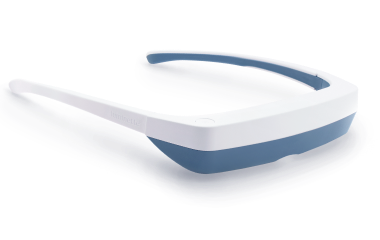
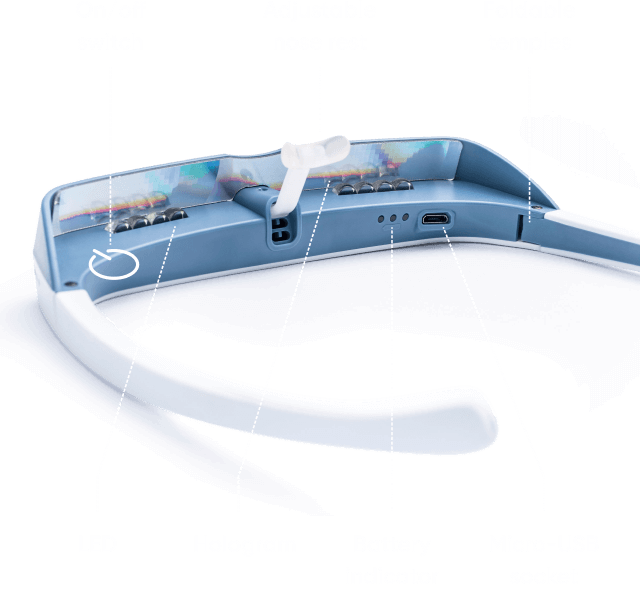
Kannettavat laitteet vähentävät myös sijoitusvirheitä. Visiirityyppisen optiikan ansiosta melanopinen annos pysyy vakaana luonnollisissa pään liikkeissä. Käyttäjät voivat valmistaa aamiaista, pakata laukkua tai lukea sähköpostia ilman, että heidän tarvitsee jatkuvasti kohdistaa valoa uudelleen paneeliin. Turvallisuus on varmistettu häikäisysuojatuilla optiikoilla, UV-vapailla LEDeillä ja maltillisella valaistuksella, kuten 2 000 luksilla silmään paneelin huippuarvojen sijaan. Tulosten osalta samanlaiset vaiheensiirrot paremmalla päivittäisellä johdonmukaisuudella voivat ylittää teoreettisesti suuremmat luksit, joita käyttäjät eivät oikeasti saavuta (Reid ym., 2018 Harvard Health, 2023.)





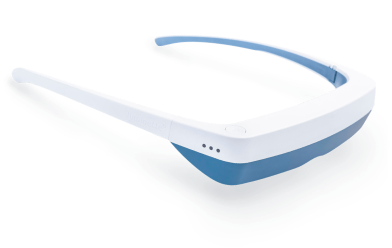
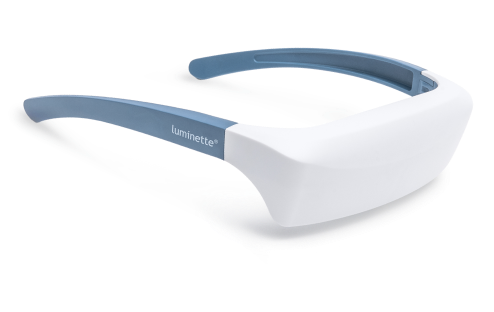
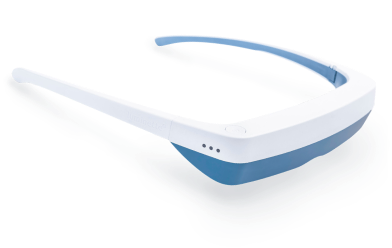
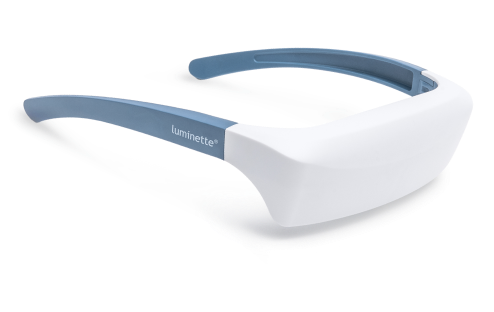
Esimerkki: Luminette 3 aamun hoitoihin
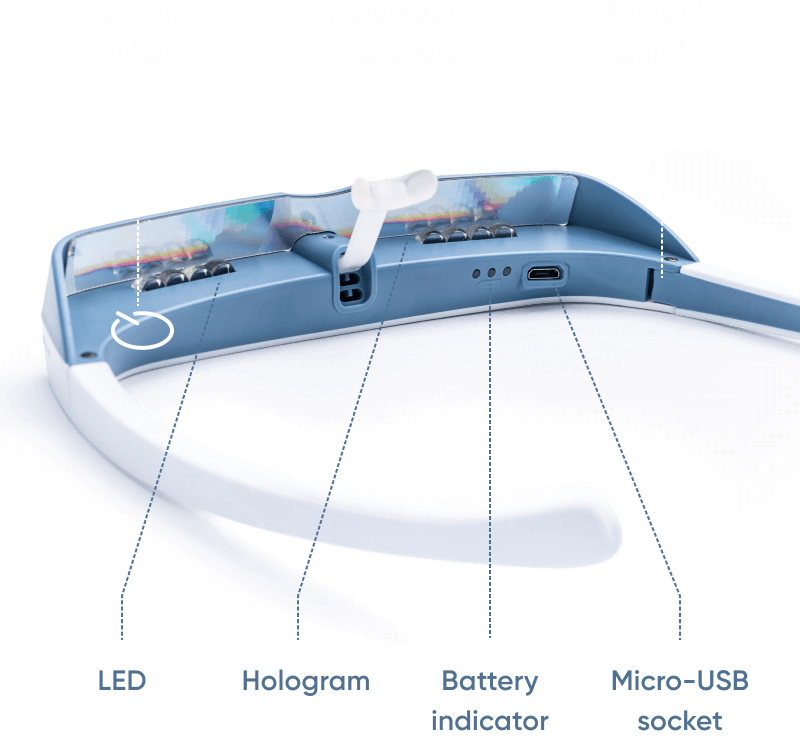
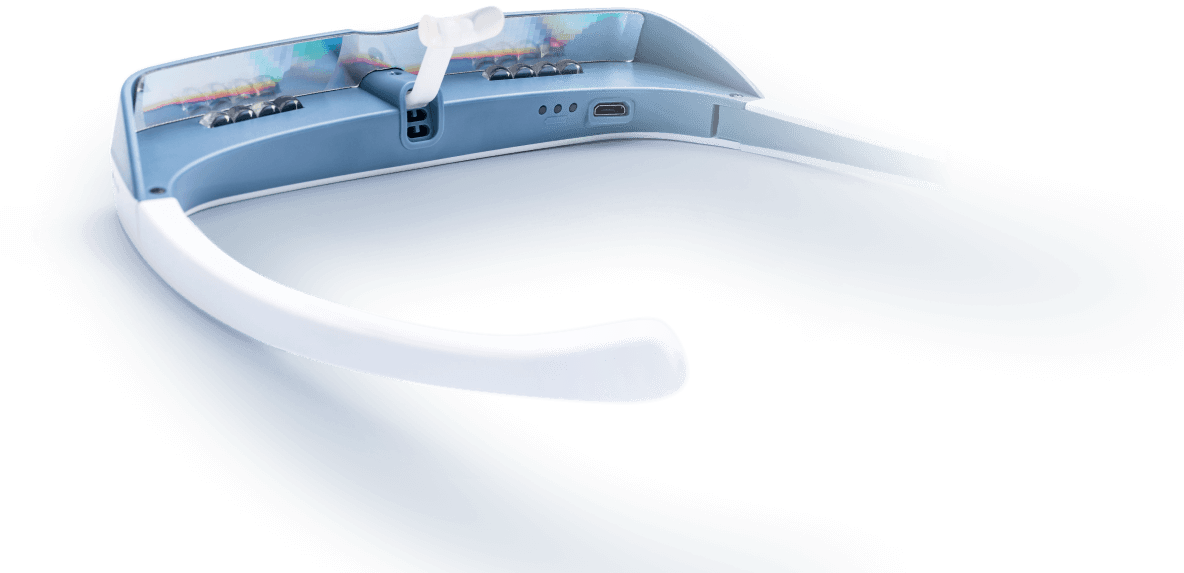
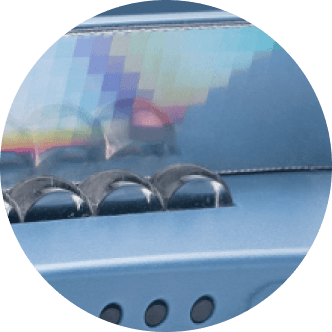
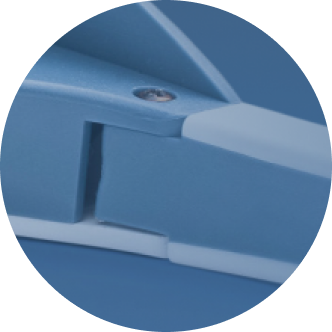
Optiikka ja annoksen toimitus. Luminette 3 käyttää yläasennettua LED-ryhmää ja diffraktiolinssejä, jotka suuntaavat sinivalkoista valoa alaspäin kohti alempaa verkkokalvoa, jossa melanopsiinipitoiset ipRGC-solut reagoivat voimakkaasti. Suunnittelu pitää valonsäteen pois suoralta näkölinjalta, säilyttäen näkökentän ja minimoiden häikäisyn samalla kun se tuottaa noin 2 000 luksin valon silmään, mikä on kliinisesti merkittävä aamun annos 20–45 minuutissa. Geometria on kiinteä kehyksen ansiosta, mikä vähentää käyttäjän virheitä ja parantaa toistettavuutta.
Käytettävyys ja turvallisuus. Koska näkö ei esty, käyttäjät voivat liikkua vapaasti. LEDit ovat UV-vapaita, optinen rakenne on säädetty mukavuuden takaamiseksi, ja ohjeistus korostaa aamun ajankohtaa. Tämä ratkaisee valohoidon suurimman esteen, eli hoidon noudattamisen, vaarantamatta biologista tavoitetta. Varhaiset kokeet, joissa verrattiin kannettavaa laitetta paikallisiin valoihin, raportoivat samanlaisia vaiheensiirtoja paremmalla hoidon noudattamisella ja käyttäjätyytyväisyydellä, erityisesti nuorilla ja kiireisillä ammattilaisilla (Rüger et al., 2020 Sleep Medicine Reviews, 2022.)
Tekstimuistiona pyynnöstä: Saatavilla on myös kannettava malli — Luminette 3 — säännöllisiin aamun valohoitoihin, joka selittää valon kompensaation luonnollisesti.
Keskeiset ominaisuudet yhdellä silmäyksellä: säädelty 2 000 luksin valo silmään, sinivalkoinen spektri, visiirin geometria kohdistaa alempaan verkkokalvoon, UV-vapaa ja heijastuksenestolinsseillä, 20–45 minuutin aamuprotokolla ja liikkumisen mahdollisuus hoidon aikana.
Kliiniset ja psykologiset odotettavissa olevat tulokset
Oikein käytettynä aamun valohoidolla on yhteneviä hyötyjä unen ajoituksessa, vireystilassa ja mielialassa. Kaamosmasennuksessa oireiden väheneminen kahden viikon sisällä on hyvin dokumentoitu. Viivästyneessä univalverytmin häiriössä vaiheensiirrot noin 1–2 tuntia ovat tyypillisiä, usein aikaisemman nukahtamisen ja helpomman heräämisen kanssa. Toimistotyöntekijät ja pohjoisten leveysasteiden asukkaat raportoivat parantunutta valppautta ja vähentynyttä aamupäivän uneliaisuutta. Vaikutukset korostuvat säännöllisyydellä, oikealla ajoituksella ja iltavalaistuksen kurinalaisuudella (Lam ym., 2016 Lewy ym., 2018 Reid ym., 2018.)
Tulokset sisältävät aikaisemman nukahtamisen ja heräämisen, vähentyneen päiväaikaisen uneliaisuuden, parantuneen reaktioajan ja työmuistin, mielialan vakaantumisen talvikuukausina, kortisolihuipun paremman ajoittumisen aamuun sekä koetun unen laadun paranemisen.
Rajoitukset, turvallisuus ja oikea käyttöaika
Valoterapia on yleisesti turvallista, mutta ajoituksella on merkitystä. Myöhäiset päivän sessiot voivat viivästyttää nukahtamista, pitkät altistukset voivat aiheuttaa ohimenevää päänsärkyä tai silmien rasitusta, ja kaksisuuntaista mielialahäiriötä tai tiettyjä silmäsairauksia sairastavien tulee saada lääkärin ohjeita haittavaikutusten välttämiseksi. Kohtele valoterapiaa kuten mitä tahansa hoitoa: seuraa vaikutuksia, säädä kestoa suositusten puitteissa ja priorisoi aamun aikavälit vaiheensiirtoa varten samalla kun suojaat iltoja kirkkaalta sinivalolta (American Psychiatric Association, 2021 Cajochen ym., 2019.)
Käytä varoen -tarkistuslista sisältää historian maniasta tai hypomaniasta, verkkokalvosairaudesta tai äskettäisestä silmäleikkauksesta, kirkkaan valon laukaisemasta migreenistä, hallitsemattomasta ahdistuksesta aktivoivien ärsykkeiden yhteydessä sekä valoherkistä lääkkeistä. Milloin ottaa yhteyttä lääkäriin: levottomuuden tai unettomuuden ilmaantuessa aamun ajoituksesta huolimatta, jatkuvien päänsärkyjen ja näköhäiriöiden ilmaantuessa, joita etäisyyden tai kulman säätö ei helpota.
Valon suunnittelu terveellisiin tiloihin: Päivittäinen valaistussuunnitelma
Yhdistä sisustus ja terapia vuorokaudenajan mukaan. Käytä aamun terapeuttista valoa kellon asettamiseen, ylläpidä kirkasta neutraalia työvalaistusta työaikana ja himmennä lämpimään hajavalaistukseen auringonlaskun jälkeen. Tätä lähestymistapaa, jota kutsutaan vuorokausikerrostamiseksi, käytetään tunnelman ja fysiologian yhteensovittamiseen, jolloin tunnelmavalot pääsevät loistamaan iltaisen rauhan aikaan ilman, että ne korvaavat kliinisen aamuisen annoksen.
Päivän aikataulutaulukko:
Aikajakso |
Tavoite |
Valotyyppi |
Esimerkki |
Aamu, 0–60 min heräämisen jälkeen |
Vaiheen aikaistus ja vireystila |
Valohoito tai sinivalkoinen, korkea luksus |
Luminette 3 -kerta 20–40 min |
Päivätyö |
Pitkäkestoinen tarkkaavaisuus |
Neutraali tai viileä työvalo, keskitasoinen tai kirkas |
4000–5000 K työpöytävalot, päivänvalotauot |
Ilta, 2 tuntia ennen nukkumaanmenoa |
Melatoniinisuoja |
Lämmin, himmeä, hajavalo |
2200–2700 K lamput, vähäinen häikäisy, ei kirkkaita näyttöjä |
Mihin ala on menossa: personoitu, adaptiivinen valaistus
Seuraava aalto on personoitu fotobiologia, jossa järjestelmät mukauttavat spektriä ja intensiteettiä kronotyypin, univelan ja vuodenajan mukaan. Tekoälyohjatut laitteet ja kannettavat koordinoivat aikatauluja varmistaen vahvan aamuisen melanopisen annoksen ja vähäisen ilta-altistuksen. Integrointi unenseurantalaitteiden ja ympäristön antureiden kanssa mahdollistaa suljetun silmukan ohjauksen, joka mittaa, mukauttaa ja säätelee (Nature Electronics, 2023.)
Nousevia trendejä ovat adaptiiviset vuorokausirytmit, melanopista tietoisuutta lisäävät spesifikaatiot, kannettavien ja kotien synkronointi, työpaikkojen päivänvalon kompensointi sekä annosteluohjelmat käyttäytymisen ohjauksella.
Yhteenveto ja käytännön vinkit
Sisustus- ja terapia-valaistus täydentävät toisiaan, eivät korvaa toisiaan. Käytä tunnelmavalaistusta tilan tunnelman muokkaamiseen ja aamuvalohoitoa biologisen kellon säätelyyn. Kiinnitä rutiinit heräämiseen, suojaa illat ja valitse laitteet, jotka ilmoittavat selvästi luksin, ajoituksen, spektrin ja geometrian.
Seuraavat askeleet ovat valita varmennettu terapiamenetelmä, aloittaa 20–40 minuutin aamukerta 30–45 minuutin sisällä heräämisestä, tarkistaa iltavalaistus lämpimäksi ja himmeäksi, lisätä lyhyitä päivänvalotaukoja sekä seurata unen alkamista ja heräämisen helppoutta viikoittain vaiheen aikaistumisen varmistamiseksi.
UKK
Voivatko tunnelmavalot korvata valohoidon?
Ei, niiden valaistusvoimakkuus on alle 500 luksin ja spektri on suunniteltu tunnelmaan, ei vuorokausirytmin säätelyyn. Terapiassa tarvitaan vähintään 2 000 luksin valo silmään ja aamun ajoitus
Kuinka pitkä terapiakerran tulisi olla?
Useimmat protokollat suosittelevat 20–40 minuuttia ensimmäisen tunnin aikana heräämisen jälkeen; johdonmukaisuus on tärkeämpää kuin maksimaalinen luksus
Onko Luminette 3 turvallinen päivittäiseen käyttöön?
aamun terapiakerrat; käyttäjät säilyttävät liikkuvuutensa, mikä parantaa sitoutumista
Toimivatko älylamput päivänvaloasetuksella?
Vain jos ne tuottavat terapeuttista luksusta silmään ja niitä käytetään aamulla protokollan mukaan; useimmat sisustuslamput ovat liian himmeitä
Entä jos tunnen oloni levottomaksi yöllä?
Tarkista iltavalaistus, vähennä kirkasta tai sinistä valoa 1–2 tuntia ennen nukkumaanmenoa, äläkä käytä terapiakertoja myöhään illalla




{kind=link}